Although the shoulder joint is the largest moving joint of the body, it is the most dislocated large joint. This joint; It consists total of five joints, as three basic and two functional. When compared to other joints, the fixation of the shoulder joint is provided by soft tissues rather than bone-bone connection. Shoulder dislocation can be considered as acute and recurrent shoulder dislocation.
SHOULDER DISLOCATION
A. ACUTE SHOULDER DISLOCATION
How and in whom Acute Shoulder Dislocation occurs?
Shoulder dislocation may occur in patients of any age group. Shoulder dislocation can often develop to forward, and rarely to back and down. The dislocation mechanism generally occurs during falls while the hand is in the open position by shoulder is being forced out. When the shoulder joint dislocates, an unbearable pain occurs with a swelling on the front of the shoulder. In this case, it is not possible for the patient to move his shoulder and arm.
At a young age a patient with shoulder dislocation for the first time; arm joint is placed to back its socket with a closed method and three weeks of arm sling use is enough for healing. In young patients, some tissues need to be torn for the development of dislocations due to their robust shoulder structures. The most common of these is, the separation of the cartilage support called labrum at its adhesion site from the bone. In addition, loosening of the shoulder capsule is one of the causes of dislocation and semi-dislocation. Due to being damaged, if the first dislocation of should age is lower than 20, re-occurring probability of shoulder dislocation is %90. However, if the first shoulder dislocation is over 40 years of age, the re-occurring probability decreases to 10%. Re-occurring dislocations; while cause detoriation in shoulder joint and arthritis, also permanent damages may occur in muscles and tendons which are around of shoulder. Also, shoulder dislocations which occur at unexpected times, causing additional disabilities. For all these reasons, surgical treatment is recommended for re-occurring shoulder dislocations.
In the elderly patient group, shoulder joint dislocations can also be accompanied by fractures. In elderly patients, these dislocations are treated surgically or under anaesthesia, and re-dislocation is unlikely except in special cases.
What Are the Symptoms of Shoulder Dislocation?
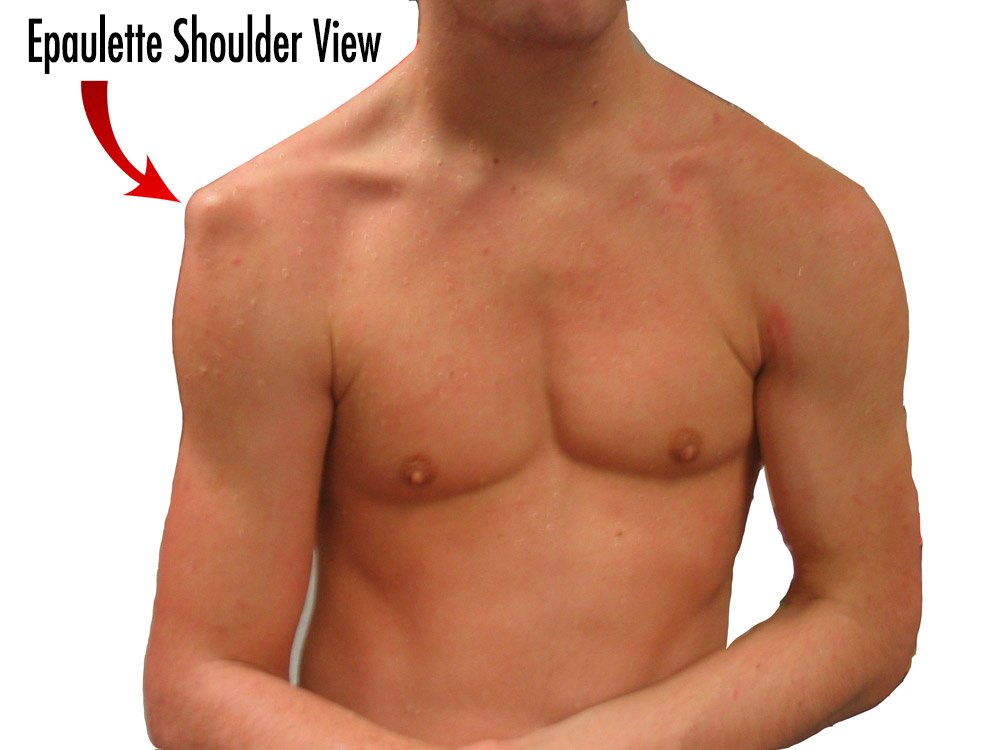
- The appearance of the deformity in the shoulder which called epaulette shoulder.
- Excessive pain presence and being unable to move the dislocated shoulder
Treatment of Acute Shoulder Dislocation
The dislocated joint should be replaced as soon as possible. Waiting for a long time will make it difficult to replace the joint, as well as disrupting the blood supply to the joint faces may cause to bone death.
The muscles should be loosened sufficiently to replace the joint. Sedation or anesthesia may be applied if this is not enough. However, if the first shoulder dislocation occurs at a young age, it is more likely to recur due to rupture of the intact structures. Surgical treatment may be preferred for the repair of the ruptured structures after the first dislocations especially in the people who are active in sports and engaged in sports professionally. Again, the treatment of 2 or more recurrent shoulder dislocations is surgery.
B. REPEATING SHOULDER DISLOCATION
1- Traumatic Dislocations
The first dislocation usually occurs after a serious trauma. Subsequently, dislocation or semi-dislocation may occur during daily activities, especially in patients under 30 years of age.
Recurrence of the dislocations may cause the patient to feel fear, anxiety of shoulder dislocation and creates a need to restrict his daily activities. Surgical treatment is required in such cases. However, recurrent shoulder dislocations can sometimes occur without tearing due to capsule looseness. In such cases, strengthening the structures around the shoulder should be tried first with physical therapy methods.
However, tendon and capsule structures that hold the shoulder joint in place are separated from the bone, especially when shoulder dislocation occurs after trauma. The head of the shoulder gets out from to joint through this torn area. This is called “Bankart Lesion”. Other structures can be damaged along with shoulder dislocation. The repair of all these damages can be treated as closed by arthroscopic method. Because of these features, such dislocations in the medical literature are also called TUBS instability consisting of Traumatic, Unilateral, Bankart lesion and Surgery initials.
90% of re-occurring shoulder dislocations are classic traumatic dislocations. In subsequent cases, dislocations can be very easy and patients usually begin to place their shoulders themselves. In this case, surgery is the only treatment option.
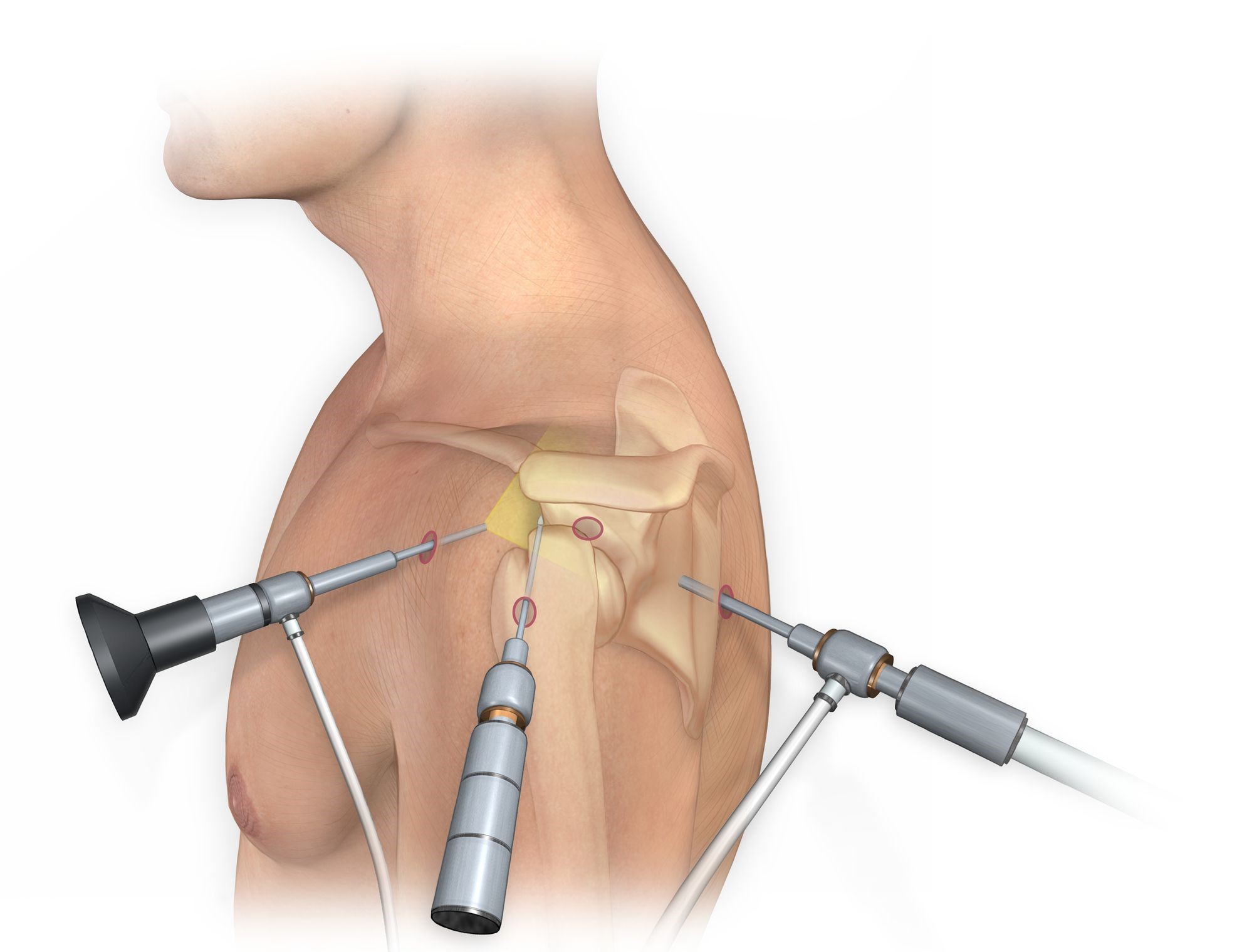
Bankart Repair with Arthroscopic Surgery
Bankart repair can be done either open or closed (ie. arthroscopic). It is the process of suturing the front labrum to its place that has been stripped from the glenoid edge’s. This process is usually done by placing anchors on the glenoid edge and sewing them into place of the labrum with the help of the sutures coming out of these anchors. After this procedure is done with closed shoulder arthroscopy, very successful results are obtained.
Arthroscopic surgeries are requiring technological equipment and very difficult procedures and requires special training. However, compared to open surgery; have many additional advantages such as; the ability to intervene in additional shoulder pathologies, short hospital stays, no need for wound care, faster tissue healing, higher patient comfort, less postoperative pain complaints, easier physical therapy, and reduced probability of limited mobility in the shoulder joint. Nowadays, arthroscopic surgery achieves around 85-90% success.
Arthroscopic surgeries are requiring technological equipment and very difficult procedures and requires special training. However, compared to open surgery; have many additional advantages such as; the ability to intervene in additional shoulder pathologies, short hospital stays, no need for wound care, faster tissue healing, higher patient comfort, less postoperative pain complaints, easier physical therapy, and reduced probability of limited mobility in the shoulder joint. Nowadays, arthroscopic surgery achieves around 85-90% success.
Shoulder arthroscopy is carried out with a camera and various instruments that are inserted in 3 or 4 holes through the joint in 1 cm size. After this operation, the arm stays in sling for 4 weeks (velpau bandage) and performing operations such as eating food and writing with the computer is become available. During this period, shoulder exercises which given 3 times a day are performed in a controlled manner. The patient can perform personal care and daily basic activities after 5-10 days. Partial active movements begin at 4-6 weeks. 6-10 After weeks, active movements are performed. After the 10th and 12th weeks, all movements except the throwing movement from the shoulder movements are allowed. After 12-16th weeks, all movements are allowed. The patient is allowed to do simple sports (sports that do not need to use the arm over the head, football and the like) in 16th week. However, if the patient is interested in sports as professional or as amateur; such as basketball volleyball or tennis, due to these sports branches are required to use the arm intensively over the head position, so the active return to these sports is after 6 months.
In cases where arthroscopic treatment cannot be performed, the torn labrum can be sutured into place with open techniques. There is no difference in tissue healing in both treatments. Open treatments are those that may require wound care and that lengthen time of stay in hospital may for several days.
2- Atraumatic Dislocations
Atraumatic Dislocations are dislocation type of; the first dislocation occurs without any significant accident, after excessive stress in daily movements (such as turning the arm, throwing, making an inverse movement), which can be seen both on the back and the front, usually seen on both shoulders, and the physical therapy is the prior treatment and which capsule narrowing operations are done in all treatment operations.
In these patients, the shoulder is easily either dislocated and relocated. 80% treatment is provided by physical therapy in good and experienced hands. Those who do not respond to physical therapy can be treated with surgical methods.
3- Intended Dislocations
Patients can intentionally dislocate their shoulders forward and back and place them in place. There are psychological reasons on the background. These patients should first give up to doing intentionally dislocation. This may sometimes require psychological treatment. However, patients with dislocation continue to receive physical therapy, if still there is a dislocation on particular movements; surgery may be tried but success rate of surgery is quite low.